Sialolithiasis is the most common disorder affecting the major salivary glands. It is an obstructive disease which results due to formation of calcified bodies within major salivary glands or within the ductal systems which drain the salivary gland. The ductal system carrying the salivary fluid is more commonly affected than body of the salivary gland. Most common site for the formation of salivary stones or calculus is the submandibular gland. The incidence of sialoliths in the submandibular salivary gland is increased due to its longer, more angled ductal system, more alkaline salivary fluid with high mineral contents and antigravity flow. The other salivary glands which are affected include the parotid and the sublingual gland.
The methods of investigation are conventional radiography (mandibular occlusal view, Oblique lateral view with reduced exposure time), CBCT, ultrasonography, computed tomography, magnetic resonance imaging, sialography.
Sialoliths which are radiolucent, are difficult to diagnose using conventional radiography. The use of sialography, color doppler, scintigraphy can help detect such radiolucent stones and/or inflammatory changes in the associated tissue within the gland. With the use of conventional sialography or CT sialography, the stone which causes obstruction to flow of the dye is visualized as a filling defect within the duct. CBCT sialography is found to be superior to conventional CT sialography in detecting calculi in the second and third order branches of the salivary glands.
CBCT imaging used in the investigation of radiopaque salivary stones is described along with related imagery in this blog.












Right submandibular ductal sialolithiasis : Axial sections and cross sections at 180µm showing localized, well demarcated, radiodense masses (2) along the lingual aspect of the right body of mandible i.r.t 42- 46 region. The region corresponds to the submandibular gland duct or Wharton's duct.
The anteriorly located mass is smaller in size and shows irregular periphery. The larger, posterior mass, extends within the lingual tissues corresponding to medial aspect of 45-46 region. It shows an oval shape with concentric structure and irregular margins. The center appears more opaque than the periphery of the mass.

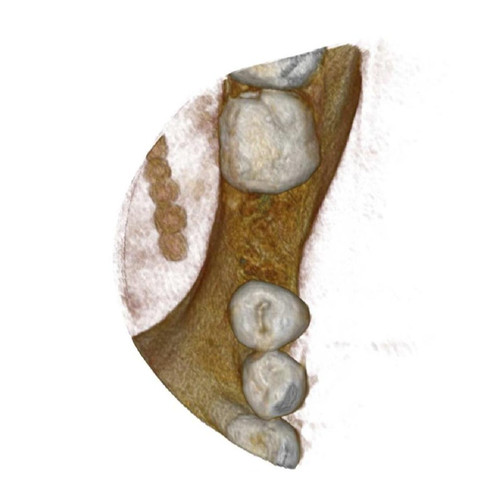



Left submandibular duct (Wharton's duct) sialolith chain : 3d images and axial sections at 90µm showing localized, well demarcated, confluent, globular radiodensities within the lingual tissues corresponding to the medial aspect of 35-37 region. The masses show a concentric pattern.


Left submandibular duct sialolith at the distal portion. Axial sections at 180µm show a localized, well defined, radiopaque mass within the lingual soft tissues corresponding to 31-33 region. The mass is located at approximately at the level of the lingual crestal region.




Calcified masses noted within left parotid gland (lower pole). Axial sections at 300µm show localized, globular radiopacities noted within the soft tissues positioned medial and lateral to the left angle of mandible corresponding to the parotid gland region.
Treatment of Sialolithiasis is dependent on the size and location of the calculus. Small calculi are treated using hydration, use of sialogogues and antibiotics. Larger sialoliths or stones located in the proximal duct are treated by Sialoendoscopy (endoscopic stone removal), endoluminal balloon dilatation and stone removal, surgical removal, piezoelectric extra/intra corporeal shock wave lithotripsy.

Thanks 👍 Dr Shikha
Thanks Dr chandan for an easy explanation of sialothosis... the diagnostic techniques are surely gonna help us come to a diagnosis....